International Claim Form Open a PDF - Updated claim form is for use starting on Jan. To make a claim and receive a payment you must file a claim form online or by mail postmarked by November 5 2021.
Https Www Bcbsmt Com Static Mt Provider Pdf Claim Bcbs Settlement Fund And Contribution Claim Form Mt Pdf
Self-Funded Account and their employees that.
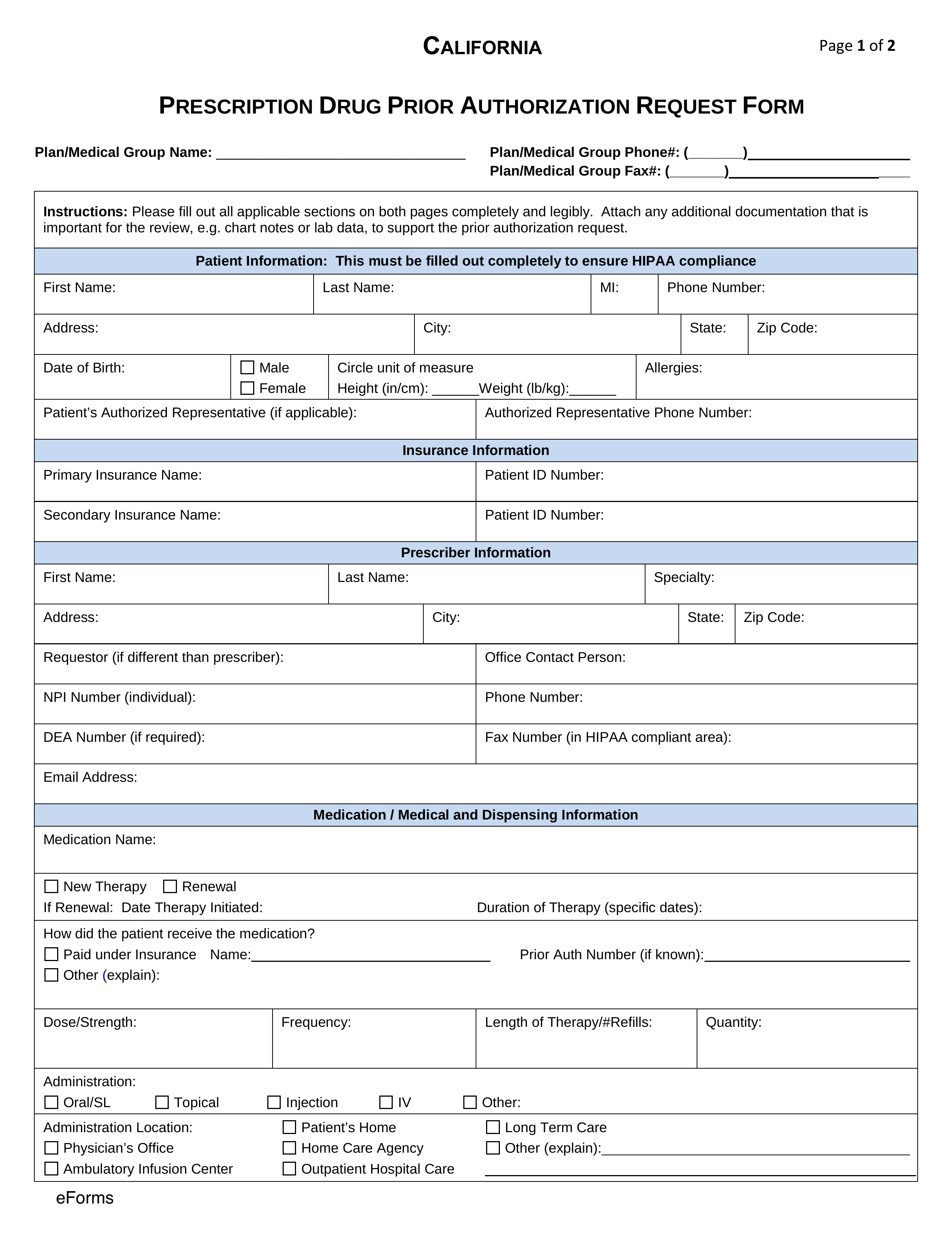
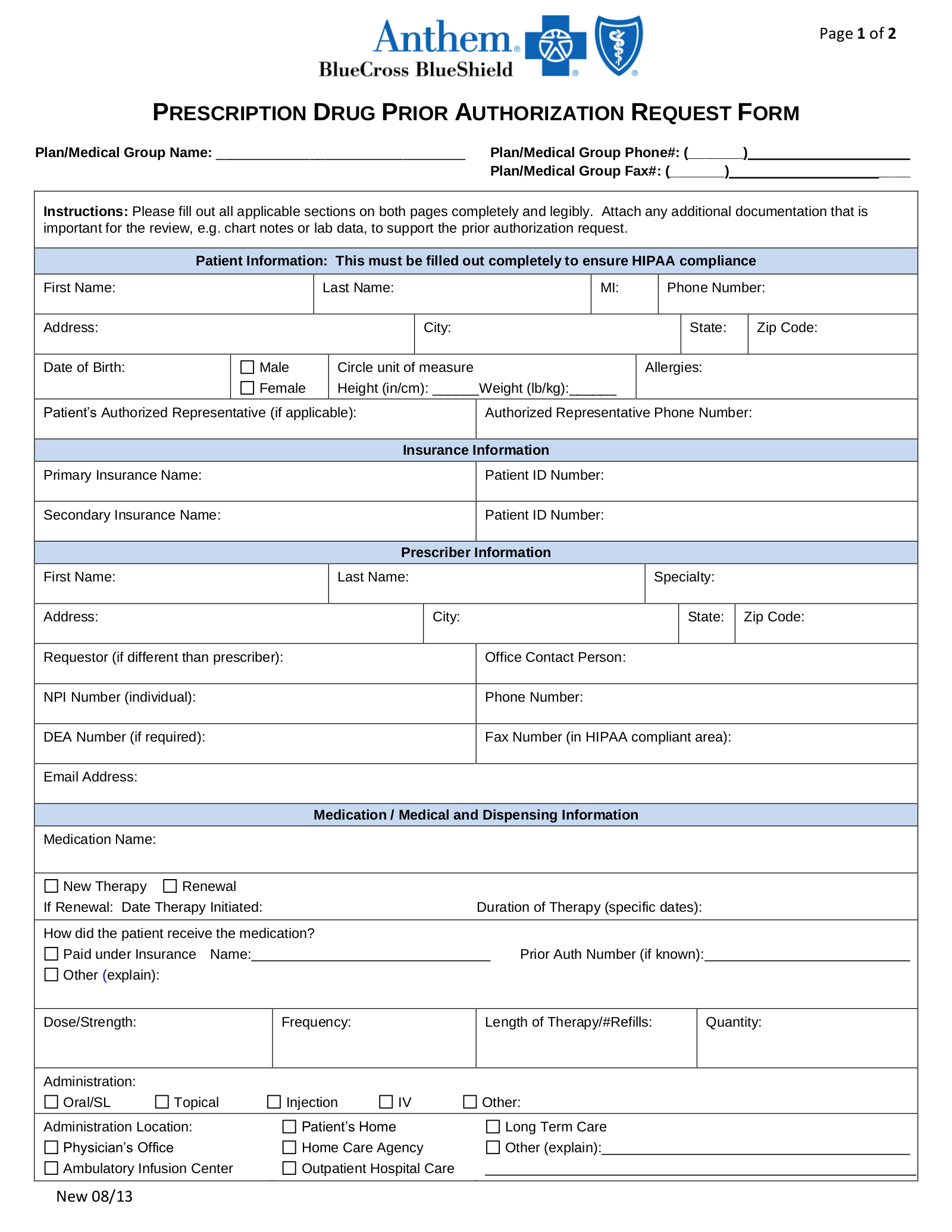
Blue cross blue shield claim form. Deluxe Item Upgrade Form. Download the dental claim form. Instructions for Submitting Claims 1.
International Claim Form in Spanish Open a PDF. Do not file prescription drugs or dental claims with this form. 1 2017 when submitting expenses incurred from rendering medical services overseas.
Check the state-by-state list of Blue Cross Blue Shield companies to get started. Long-Term Disability Claim Form. Blue Cross Blue Shield Global Core Claim Form offsite link Cancer Plan Claim Form Form 29-134 Claim Appeal Form Form 34-730WEB Spanish version Claim Appeal Representative Authorization Form Form 29-58 Hospital Indemnity Plan Claim Form Form 29-142 Member Claim Form to include prescription drugs processed by BCBSKS.
To file a claim for 2019 coverage use this Prescription Drug Claim Form. Long-Term Disability Claim Form - Spanish. Use this form to select an individual or entity to act on your behalf during the disputed claims process.
Blue Cross and Blue Shield of Illinois PO. Prescription Drug Claim Form. BLUE CROSS BLUE SHIELD CLAIM FORM.
Blue Cross Blue Shield Settlement CO JND Legal Administration PO Box 91390. Blue Dental Out-Of-Network Claim Form PDF File. Please complete every item on claim form.
Individual Insured Group and their employees or. Write your BlueCross BlueShield. Use the Prescription Drug Mail Service Form.
If you go to an out-of-state doctor or hospital that doesnt participate with Blue Cross Blue Shield you may pay upfront for services. Blue Cross Blue Shield Global Claim Form. Form Title Networks Expedited Pre-service Clinical Appeal Form.
Insurance products issued by Dearborn Life Insurance Company 701 E. Medical Claim Form International Use this Blue Cross Blue Shield Global Core International Medical Claim form to request reimbursement for applicable medical expenses incurred internationally for services not directly billed to the plan. However if you need to file a paper claims use one of the following claim forms.
Blue Cross Blue Shield Settlement co JND Legal Administration PO Box 91390 Seattle WA 98111. You may be eligible to receive a cash payment if you are an. CMS-1500 form for all other charges Tips for paper claim submission.
Long-Term Disability Conversion Kit. Medicaid Claims Inquiry or Dispute Request Form. Claims may be submitted online or by mail to.
Submit a separate form for each patient. You can fill the form in electronically or complete it by hand Print and mail the form to your local Blue Cross and Blue Shield company by December 31 of the year following the year you received service. Find your local companys address.
Authorized Representative Designation Form. With this benefit you can order up to a 90-day supply of your prescriptions. Short-Term Disability Claim Form.
Waiver of Premium Claim Form. UB04 form for hospital charges. Medicaid only BCCHP and MMAI Medicaid Service Authorization Dispute Resolution Request Form.
Box 805107 Chicago Illinois 60680-4112. Claims should not be submitted before the effective date. If you regularly take medication you may also want to look into our mail-order service.
You must sign the claim form certification in Section F and mail it to the address below postmarked by November 5 2021 in order for your claim to be considered. When filing a Medicare Supplement claim follow these steps. Member Claim Form Requirements Please note the below filing requirements and tips for filling out the attached Member Claim Form.
Short-Term Disability Claim Form - Spanish. Submit a claim only when you are billed for services from a provider that does not directly submit a claim to the local Blue Cross Blue Shield plan. To file a claim for those out-of-network services youll need to use the claim form from the state where you were treated.
Attach an original itemized bill from your provider required information example on the back 4. Suite 300 Lombard IL 60148. Were enrolledin a Blue Cross.
Blue Cross and Blue Shield of Texas is the trade name of Dearborn Life Insurance Company an independent licensee of the Blue Cross and Blue Shield. You can find detailed instructions on how to file an appeal in the Disputed Claims Process document. After completing the appropriate form mail it to the address shown on the back of your patients Blue Cross NC member ID card.
Do NoT file this form if your Provider of Service is submitting these charges to Blue Cross and Blue Shield of Illinois. Spanish Version PDF File. English Version PDF File.
Complete the form following the instructions on the back. In these cases use the Prescription Drug Claim Form. Blue Cross Blue Shield Global Core International Claim Form Request to Authorize Payment of a Foreign Drug Claim Subscriber Claim Form.
This completed form together with the itemized bills should be submitted to. Medicaid only BCCHP and MMAI. Or Blue Shield BCBS health insurance or administrative services plan during one of the two Settlement Class Periods.
Blue Dental Extra Dental Cleaning Enrollment Form PDF File If your plan offers a 3rd annual cleaning and you are pregnant or have diabetes you can use this form to apply.