The California State Disability Insurance SDI program provides short-term Disability Insurance DI and Paid Family Leave PFL wage replacement benefits to eligible workers who need time off work. PDF fill-and-print forms may be completed online and printed to hardcopy to be signed and mailed in or submitted in person to an eligibility worker for.
 Free 8 Sample Disability Application Forms In Pdf
Free 8 Sample Disability Application Forms In Pdf
For those forms visit the Online Forms and Publications section.

Medical disability forms california. California Business and Professions Code BP section 24365 requires licensees to pay a mandatory fee of 2500 at the time of renewal of a physicians and surgeons license to the Physician Loan Repayment Program. Completing disability evaluation forms 1- 1. Mc 017fmc 017 sp - what you should know about your medi-cal disability application 1 2.
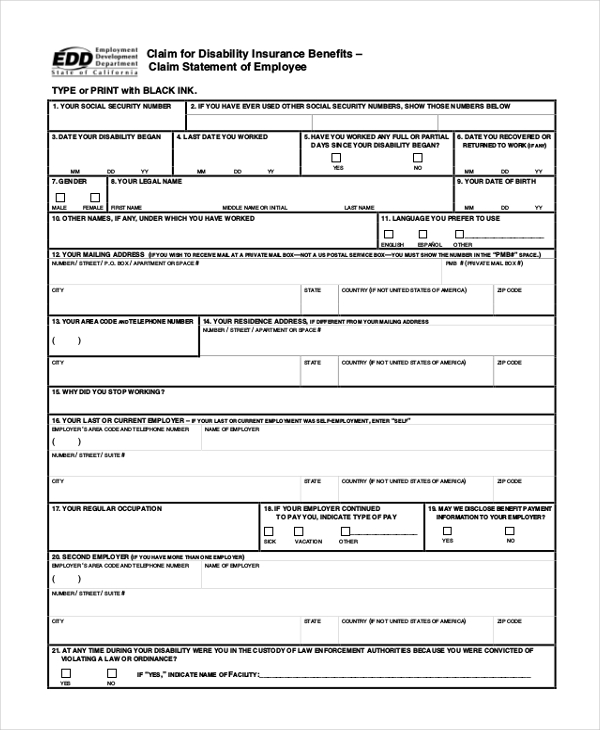
Complete and sign the Claim for Disability Insurance Benefits-Religious Practitioners Certificate DE 2502 in lieu of Part D PhysicianPractitioners Certificate of the Claim for Disability Insurance DI Benefits DE 2501 before sending it to the EDD. We may be able to help with costs such as ongoing visits to the doctor medicines medical alarms and travel. For a list of translated MCED forms by language please click on the following link.
Be able to get extra help through a Disability Allowance. Learn more about these rights in the resources below. Follow these instructions to file a Disability Insurance DI claim online to the California EDD.
Recent legislation effective January 1 2021 expands CFRA in several major respects. If you need help with this form call us on 0800 559 009. Mc 179fmc 179 sp - 90-days status lelter 3.
This includes medical records doctors reports and recent test results. Have not been denied for disability in the last 60 days. Under sections 2116 and 2122 of the California Unemployment Insurance Code it is a violation for any individual who with intent to defraud falsely certifies the medical condition of any person in order to obtain disability insurance benefits whether for the maker or for any other person and is punishable by imprisonment andor a fine not.
An Adult Disability Report that collects more details about your illnesses injuries or conditions and your work history. You must submit an original form provided by the EDD either electronically or through US mail. SDI Forms and Publications Disability Insurance Forms.
Disability Insurance and Paid Family Leave Benefits. Medi-Cal Eligibility Division Forms. Check out results for Medical disability forms in London.
You develop a notifiable medical condition or disability. Do not complete these forms if you are a licensed physician or practitioner. Some forms and publications are translated by the department in other languages.
You can use the online application to apply for disability benefits if you. Are not currently receiving benefits on your own Social Security record. Visit Online Forms and Publications to search view and order State Disability Insurance forms.
Mc 222 laimc 222 oak - dapd peyding information update. Are age 18 or older. This form must be completed by a physicianmedical specialist who specializes in your disabling condition.
W-2 formss andor self-employment tax returns for last year. It cannot be downloaded or reproduced. Medical evidence already in your possession.
You must tell DVLA if you have a driving licence and. You may be eligible for DI if you are unable to work due to non-work-related illness or injury pregnancy or childbirth. Are unable to work because of a medical condition that is expected to last at least 12 months or result in death.
To submit the DE 2501 electronically visit How to File a Disability Insurance Claim in SDI Online. Please read this before you start. Mc 220 - authorization for release of medical information 5.
Medi-Cal Eligibility Division MCED forms are listed below by form number. To complete forms you may need to download and save them on the computer then open them with the no-cost Adobe Reader. In addition California law requires covered employers to provide employees disabled by pregnancy childbirth or a related medical condition with unpaid job-protected leave PDL andor accommodations.
Forms Claim for Disability Insurance DI Benefits DE 2501 English. A condition or disability has got worse since you got your licence. Your doctor or specialist will need to complete the Disability Certificate.
Forms and publications provided on the EDD website cannot be translated using Google Translate. The Physician Loan Repayment Program encourages recently licensed physicians to practice in underserved locations in California by authorizing a plan of repayment of their medical. The following information is needed in connection with the patients application for disability retirement benefits under the California Public Employees Retirement Law.