The form must be completed in its entirety. Missouri Medicaid Prior Rx Authorization Form Department of Social Services DSS MO HealthNet Division phone number.
Https Www Healthnet Com Static Pharmacy Provider Medicare Pa Form Pdf
Non-network providers are encouraged to submit online as electronic requests save time and improve accuracy.
Health net medication prior authorization form. All information must be supplied or the request will not be processed. Day week month Total Units. Prior Authorization for MassHealth Providers.
HSP Prior Authorization Check. Day week month Total Units. Required clinical information - Please provide all relevant clinical information to support a prior.
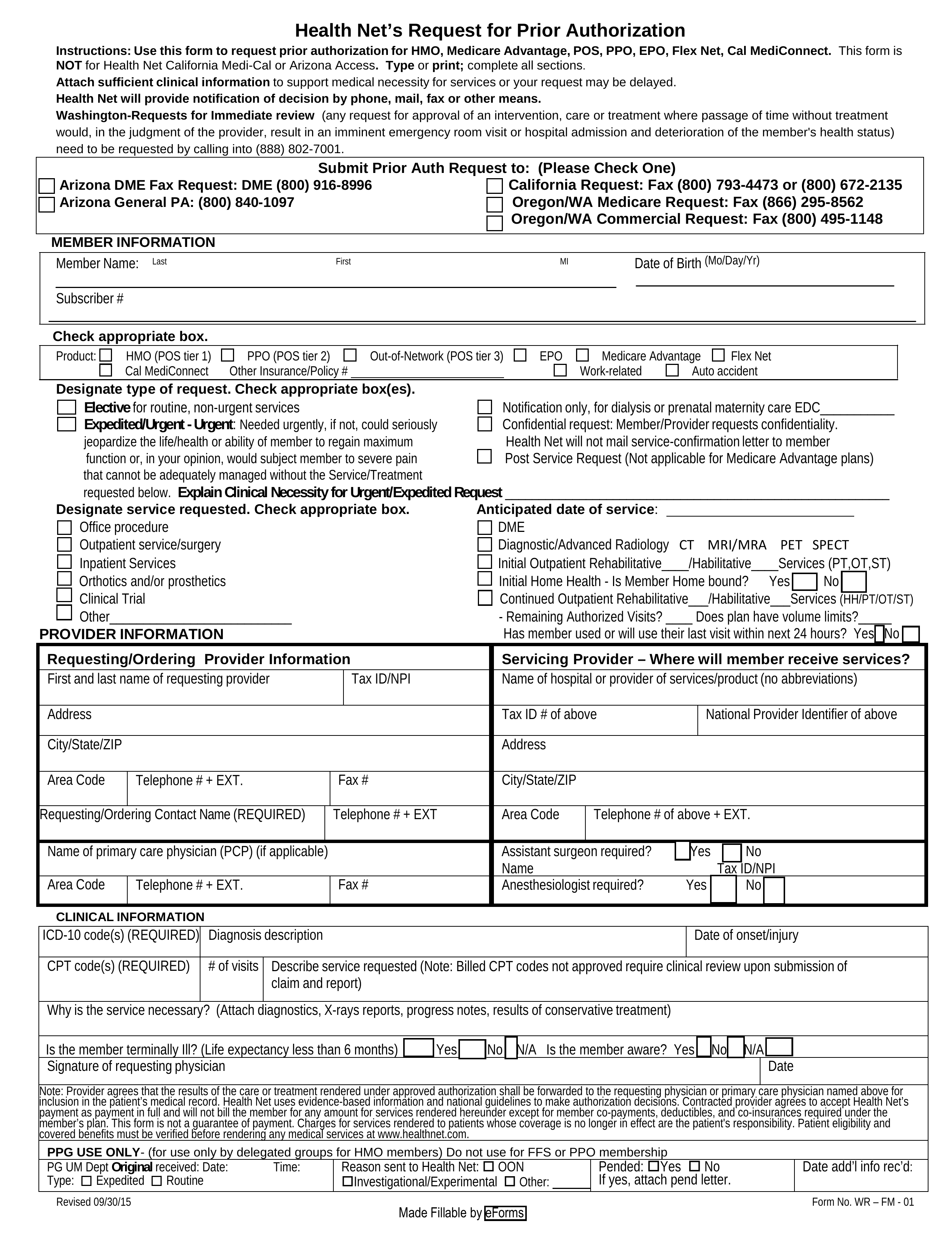
Fax 1 800 793-4473 or call 1 800 672-2135 OregonWA Medicare Fax Request. If you believe that it is medically necessary for a member to take a medication excluded by our pharmacy program and you have followed the procedures required by our pharmacy programs you may request a coverage review. We may not cover the drug if you dont get approval.
1 800 392-8030 Form can be faxed to. Prior Authorizations Prior authorizations for certain services andor procedures require Health Net Federal Services LLC HNFS review and approval prior to being provided. Prescription prior authorization forms are used by physicians who wish to request insurance coverage for non-preferred prescriptions.
Check to see if we offer a Letter of Attestation you can attach instead of clinical documentation. PA information for MassHealth providers for both pharmacy and nonpharmacy services. 1 866 295-8562 OregonWA Commercial Fax Request.
Please fill out all applicable sections completely and legibly. PPO Prior Authorization Check. HMO Prior Authorization Check.
On the prior authorization form the person making the request must provide a medical rationale as to why the chosen. For questions call 952-883-5813 or 800-492-7259. Select the members plan below to get started.
211 Zeilen MO HealthNet utilizes a real-time prior authorization rules engine in order to. This is called prior authorization. Prior Authorizations Request prior authorization for a medication.
Network providers requesting prior authorization for an elective admission or submitting an inpatient admission notification are required to submit online. 800-424-7640 2017 2018 Magellan Health Inc. This will expedite the review process.
08222018 CAT0029 Page 1 of 3 Instructions. Medical Drug Prior Authorization Form Fax form to. Medi-Cal Prior Authorization Request Form Inpatient PDF CalViva Health Prior Authorization Request Form Outpatient PDF CalViva Health Prior Authorization Request Form Inpatient PDF Online Prior Authorization Validation Tools.
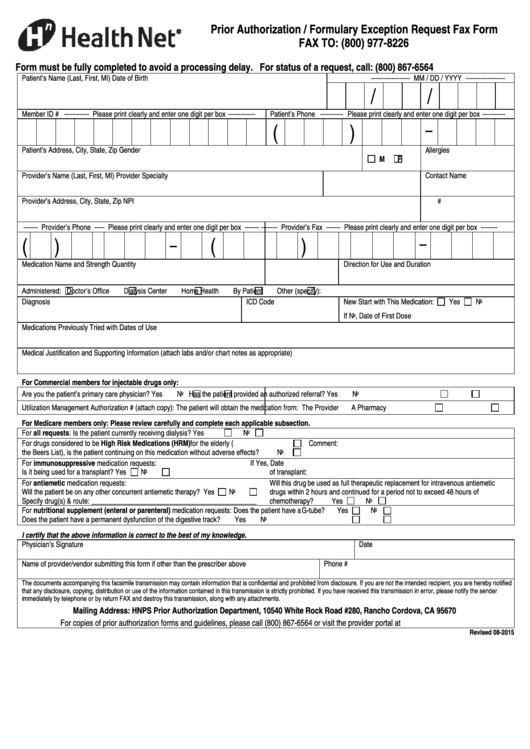
A non-preferred drug is a drug that is not listed on the Preferred Drug List PDL of a given insurance provider or State. Prior Authorization Correction Form. To request prior authorization your prescriber must complete and fax a Prior Authorization form to 1-800-314-6223 for Commercial members or 1-800-977-8226 for Medi-Cal members.
3138716229 Product Information Medication. Adhd medication prior authorization children less than 6 years old. Simply select the beneficiarys TRICARE plan option for example TRICARE Prime or TRICARE Prime Remote the beneficiary type for example active duty service member servicing provider type for.
View Our Prior Authorization Guidelines. 1 573636-6470 Form can be mailed to. Magellan Rx Management Commercial Clients.
1 800 840-109 California Request. The Prior Authorization Correction Form is to be utilized to request changes to an existing Prior Authorization. Pharmacy Administration - Prior Authorization Exception Form.
Drug prior authorization mo healthnet division po box 4900 jefferson city mo 65102-4900. Box 4900 Jefferson City MO 65102-4900. The Prior Authorization Referral and Benefit Tool allows you to easily determine if an approval from Health Net Federal Services LLC HNFS is required.
FAX to 952-853-8700 or 1-888-883-5434. Inpatient TRICARE Service RequestNotification Form. Will waiting the standard review time seriously jeopardize the life or health.
Please print or type. Drug Prior Authorization MO HealthNet Division PO. Prior Authorization Request Form Caterpillar Prescription Drug Benefit Phone.
Any additional medical documentation for this request should be submitted with this request. DME 1 800 916-8996 Arizona General PA. PRIOR AUTHORIZATION REQUEST FORM For authorization please answer each question and fax this form PLUS chart notes back to the U of U Health Plans Prior Authorization Department at 8885098142.
Health Net Prior Rx Authorization Form Arizona DME Fax Request. Failure to submit clinical documentation to support this request. Incomplete or illegible submissions will be returned and may delay review.
 2011 Health Net Prior Authorization Formulary Exception Request Fax Form Fill Online Printable Fillable Blank Pdffiller
2011 Health Net Prior Authorization Formulary Exception Request Fax Form Fill Online Printable Fillable Blank Pdffiller
Https Www Healthnet Com Content Dam Centene Healthnet Pdfs Provider Ca Hn Npo Training Guide Ucd Pdf
 Fillable Online Health Net Medicare Prior Authorization Form Pdf Fax Email Print Pdffiller
Fillable Online Health Net Medicare Prior Authorization Form Pdf Fax Email Print Pdffiller
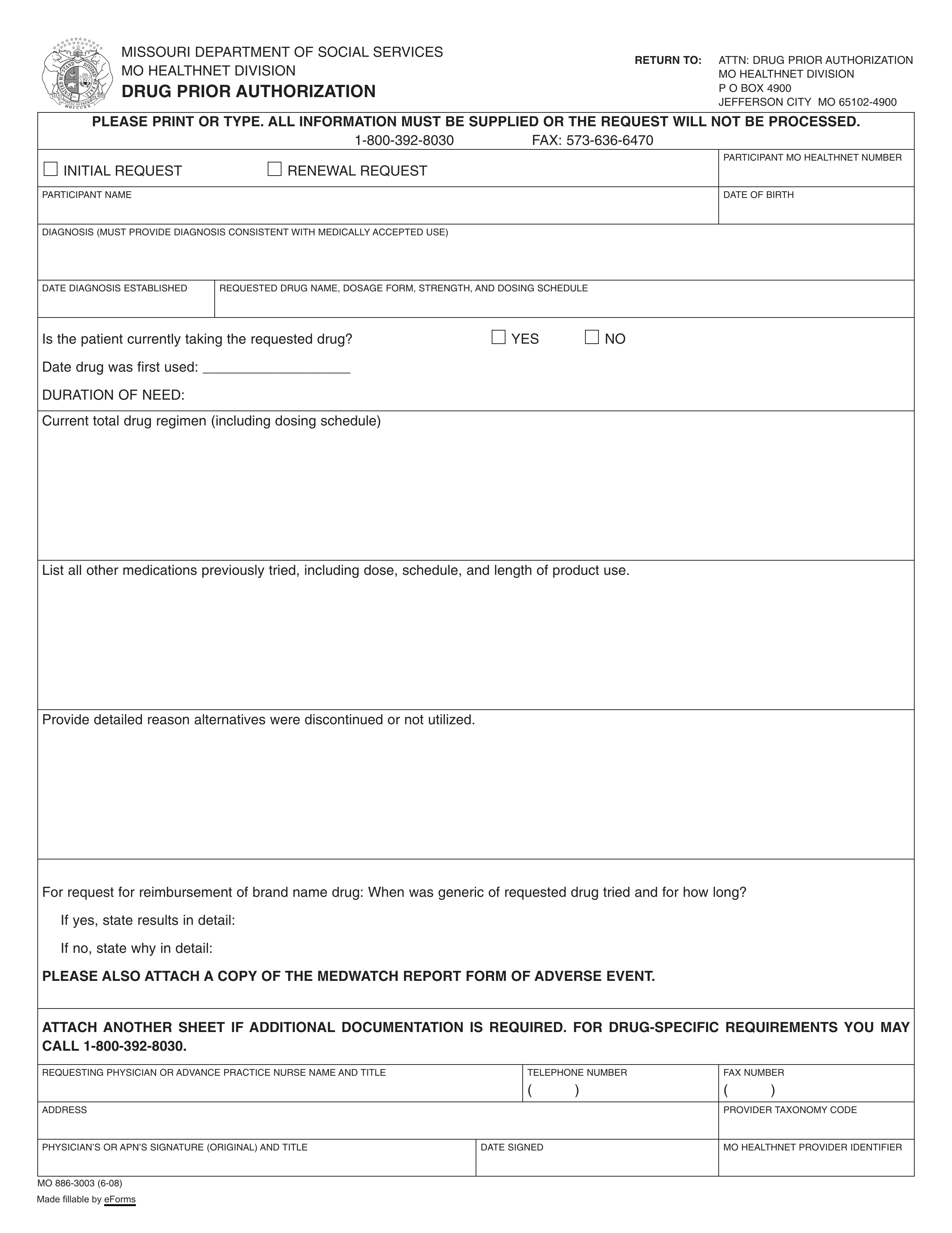 Free Missouri Medicaid Prior Rx Authorization Form Pdf Eforms
Free Missouri Medicaid Prior Rx Authorization Form Pdf Eforms
 Pharmacy Prior Authorization Form Medical Necessity Health Net Fill Out And Sign Printable Pdf Template Signnow
Pharmacy Prior Authorization Form Medical Necessity Health Net Fill Out And Sign Printable Pdf Template Signnow
 Free Health Net Prior Rx Authorization Form Pdf Eforms
Free Health Net Prior Rx Authorization Form Pdf Eforms
 Health Net Prior Authorization Formulary Exception Request Fax Form Printable Pdf Download
Health Net Prior Authorization Formulary Exception Request Fax Form Printable Pdf Download
Https Healthnet Com Static General Unprotected Pdfs Or Pharmacy Prior Auth Request Form Pdf
Https Www Healthnet Com Static Medicare Misc Form Exception Member Ca Pdf
 Bmc Prior Auth Form Fill Online Printable Fillable Blank Pdffiller
Bmc Prior Auth Form Fill Online Printable Fillable Blank Pdffiller
 Fillable Online Pharmacy Prior Authorization Form Fax Health Net Fax Email Print Pdffiller
Fillable Online Pharmacy Prior Authorization Form Fax Health Net Fax Email Print Pdffiller
Https Www Healthnet Com Provcom Pdf 30919 Pdf
 Free Prior Rx Authorization Forms Pdf Eforms
Free Prior Rx Authorization Forms Pdf Eforms
Https Www Healthnet Com Content Dam Centene Healthnet Pdfs Pharmacy Ca Ca Universal Pa Form Pdf




No comments:
Post a Comment
Note: Only a member of this blog may post a comment.